- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Telehealth and Pain Medicine
- Home
- Back to Journal
- Article Details
Buzz words like telemedicine, teleclinics, e-health, and virtual medicine are unavoidable at the moment. However, the use of remote technology platforms in medicine is not a new concept. In 2012, McGeary et al. [1] recognised that the use of telehealth (defined for the purposes of this paper as technology that allows for distance interaction between providers and/ or patients) to assist in pain management would become part of the natural progression. In 2018, the European Commission predicted the global telemedicine market would reach €37 billion by 2021. It also estimated an annual growth rate of 14 per cent [2]. Within this market medical consultations will continue to be the key growth area as clinicians use technology to provide outreach advice. The telemonitoring segment will also be an important growth area [2].
In the current public-health crisis, not only are online services experiencing renewed interest but they are playing a vital role in continuing to deliver healthcare services to patients who either can’t or are reluctant to attend their doctor’s surgery in person. However, the inclusion of a telehealth platform within a pain management service is not without its own issues.
Fast-Tracking of the TeleHealth Option
The literature warned clinicians to “develop telehealth pain services to fit patient needs, not technological advances” [1]. Cost analysis and patient expectations were regarded as important factors and providers were advised to be “mindful of their treatment targets” in order that telehealth technology can meet “patient treatment expectations” [3].
Pre-COVID19 a gradual organised approach was seen as the best way forward and a mixture of reticence, regulations and technical ability led to a slow adoption in Europe. The COVID-19 pandemic has shifted the goal posts. The gradual organised approach proposed in the early years has been replaced with the need to quickly provide support across the healthcare systems. The need to support individuals with non-urgent and long-term conditions at a distance by a variety of healthcare providers has become imperative. Chronic pain patients need to benefit from these changes. The “expectations of the patient” has also changed [3, 4]. In the April edition of PAIN, Eccleston et al. 2020 [4] felt that pain clinicians needed to adapt to the situation citing population demand and the impact of not treating chronic pain as significant factors. In fact, the field of telehealth offers a novel opportunity to expand pain assessment, consultation, and treatment services beyond the walls of the pain clinic [5].
The challenge
In the present healthcare model, the patient pathway is a simple two-step process; (a) The majority of pain management is delivered “face-to-face” and physical examination is seen as an important aspect to help identify the primary source of pain; (b) Over 80% of individuals who attend a pain consultant for the first time are likely to require a pain intervention / injection to optimise the therapy.
Two issues have arisen in the present public health crisis; firstly elective, routine, and nonemergency casework has stopped. This has delayed those who were expecting treatment and for individuals seeking their first pain consultation they are likely to be waiting an additional 6–9 months. The average wait time for a public patient to see a pain consultant is already 2 years. Secondly, the population with the higher incidence of chronic pain (e.g., older age, lower socioeconomic status, smoking prevalence, chronic disease comorbidity, and limited access to health care) are also those most effected by the COVID pandemic [4, 5].
Combine these two issues with the fact that when people with chronic pain are denied assessment and treatment, their condition can worsen significantly [4]. Therefore the challenge is to ensure that pain management becomes available to those who need it in a timely fashion [6].
Recognition Requires Review
The high prevalence of chronic pain combined with the fact that spontaneous recovery from chronic pain is rare ensures that individuals with chronic pain have the largest global morbidity, measured by years lived in disability [7].
Even as the restrictions are lifted delays in the patient care pathway are unavoidable due to the impact of social distancing guidelines; limits will be imposed on the number of individuals who can attended outpatient clinics; the number of interventional options will be reduced, the ability of physiotherapy, occupational therapy and psychology services to operate will be reduced. The best educated guess is that functional capacity of pain services will been reduced by 50–70% with immediate effect. This delay in seeing individuals with pain is known to result in levels of pain that interfere with their ability to function, and reports of severe pain are associated with more severe levels of depression in 50% and suicidal thinking in 34.6% [8]. Furthermore, people waiting over 6 months for assessment experience deteriorating health-related quality of life, increased pain, and increased depression [9].
This reduction in the capacity comes with other risks. The risk of harm from undertreatment can be exacerbated further by the risk of harm from inappropriate treatment. In many countries, for example in the United States and Canada, chronic pain management is practiced in the “shadow of a crisis of the oversupply and overuse of opioids” [10]. Referral to pain clinics for pain medicine management is common [11] but referring everyone for opioid stewardship is unrealistic [12]. In North America, there is an increase in serious mental health problems as some turn to illicit sources of opioids, while others suffer in silence [13]. Not treating chronic pain will have consequences for individuals, healthcare systems, and providers in the short- and long-term, increasing quantity, severity, and complexity of need.
What does Telehealth Technology offer Pain Medicine?
Assessing pain clinically relies heavily on what symptoms the patient reports. For example the descriptive language used by the individual can help identify between an inflammatory source of pain or neuropathic pain. The pain intensity can be scored and the aggravating factors listed. The distribution of the pain can identify the effected nerve root or roots. The disturbance in sleep, ability to walk, even the ability to concentrate are all dependant on how the individual feels the pain impacts on their functional capacity and ultimately their quality of life. Subjective assessments can sometimes be captured where there are validated reliable questionnaires to assist in this assessment but essentially it is the clinician’s impression of the patient’s symptoms that is important.
Even aspects of physical examination can be assessed virtually. For example, the gross appearance, posture or range of movement can all be demonstrated and to the trained clinician a lot of valuable information extracted. Certainly the lack of a physical hands-on examination may limit the differential diagnosis but a modified virtual assessment can allow for some initial treatment planning to commence.
Mobile telephones or devices with camera technology allow for shareable images of paper assessments or live demonstrations. Several web-based systems have been optimised for people with pain, such as the CHOIR system in the United States [14] or the PAIN OUT system in Europe [15].
There are many certified IT providers, who provide the platforms to allow safe and effective data transfer and there are many options to subscribe to these technology providers.
Evidence for Efficacy of TeleHealth
Over the years the expansion of internet and smart mobile phones with a camera has brought the real possibility of using of technology in the healthcare setting. If the number of research articles published on PubMed were to be used as barometer of how fast this area is growing then between 2012 and 2019 the number of publications doubled with 3,189 papers on PubMed in 2019 [16]. Only 3.5% of the publications were telehealth studies associated with pain during the same period with the highest number of papers published peaking last year at 112 papers (Figure 1) [16].
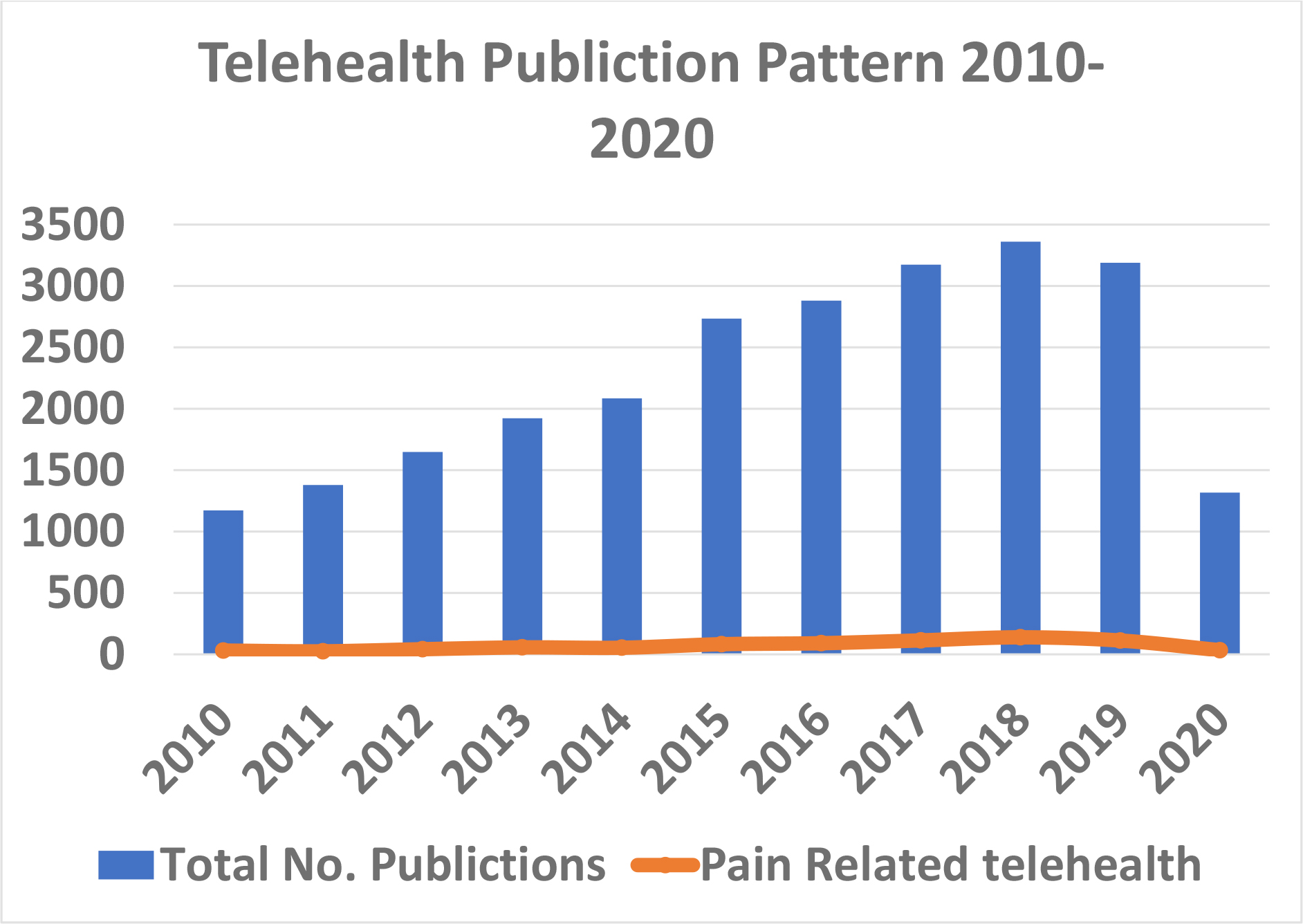
Figure 1: shows the number of papers published in PUBMed annually over the last 20 years on telehealth in medicine. Pain Medicine only contributes 3.5% of the total number.
When compared to other areas pain medicine has fallen behind in adapting a role for telemedicine. Most of the innovations have been in the development of internet-based programs. For example there are many examples of on-line programmes helping to deal with pain [17]. Eight years ago the editor of Pain Practise in 2012 comments that whether we like it or not telemedicine “is here to stay” [1]. The need generated by the COVID pandemic could be seen as the catalyst to fast-track the option. Since McGeary et al. [1] first focused on this area several reviews have followed. The reader is referred to several systematic reviews which have been published since then [11, 18–20].
The common theme of all these reviews is that they highlight small to moderate reductions in pain, disability, and distress in intervention groups compared with any control (including active, standard care, or wait list control) [11, 19].
This is at least reassuring that remote pain medicine when compared to face-to-face treatment showed no negative difference in treatment effect between remote and in-person therapies [19]. Remotely delivered physical exercise interventions are also assessed, with benefits comparable with usual care for reducing pain and beneficial compared with no treatment.
In the setting of a pandemic there is one fundamental difference, namely the option of a face-to-face consultation is effectively removed so individuals in chronic pain will value the input from their consultant even more.
Concerns
There are some concerns that must be recognised related to the use of telemedicine in pain medicine [4]. For example there are relatively few studies assessing for possible harm, and the dropout rate from on-line programmes use can be substantial. Access and engagement are important to track and report, particularly in disadvantaged groups such as older adults or disabled people who to date have used technology less [4]. When language is a barrier the use of an interpreter to communicate third hand is untested.
Understanding who struggles to engage with and how they use the telehealth system provided is crucial to maximise effectiveness. Concerns about privacy, transparency (e.g., therapist-generated vs automated messages), and training needs of staff accustomed to face-to-face working have to be consider but are not insurmountable.
Although communication technology is relatively inexpensive there will be issues regarding installation costs [2]. Telephone consultations are easy but can be very limiting. Many clinics will not have enough suitable computer terminals with cameras or tablets to meet the immediate restructuring that is required. Software updates, and the licencing costs, to keep up to the changing demands of telehealth technology will need investment. Then there is the issue of broadband capacity of a hospital, or primary care centres to deal with the increase in traffic on the server. A poor signal or audio connection, which are sometimes an issue in more remote centres, will undermine the confidence of all concerned. The ability to provide user friendly “apps” to allow smooth ease of access between the patient and pain team needs to be considered. Fortunately there are several IT firms with solutions already available in the marketplace. The day of the healthcare worker taking out his or her private mobile to “facetime” is long gone.
Final
The long-term impact of the COVID-19 pandemic is likely to reshape the way we manage all aspects of medicine. The consequences for people with chronic pain, who represent a large population with the greatest global burden of disease has yet to be modelled but they are likely to be substantial. With social distancing measures likely to be in place for some time to come the growth of Telemedicine and related eHealth interventions for pain medicine will be an important tool in any pain service. Ubiquitous communication technology is relatively inexpensive to access. Practically, the infra-structure must be available for this to work and all the relevant stakeholders must be invited to part-take to provide the solutions. We need to take the opportunity to learn from this abrupt change in our practice in order to develop research priorities to improve the evidence that telehealth sector can offer pain management.
Hegarty D.A. (2020) Survey of pain related telehealth papers on PubMED 2000–2020.
References
- McGeary DD, McGear CA, Gatchel RJ (2012) A comprehensive review of telehealth for pain management: where are we and the way ahead. Pain Pract 12: 570–7. [View]
- https://www.marketdataforecast.com/market-reports/europe-telemedicine-market
- Rosser BA, McCullagh P, Davies R, Mountain GA, McCracken L, Eccleston C (2011) Technology-mediated therapy for chronic pain management: the challenges of adapting behaviour change interventions for delivery with pervasive communication technology. Telemed J E Health 17: 211–216. [View]
- Eccleston C, Blyth F, Dear BF, Fisher E, Keefe FJ (2020) Managing patients with chronic pain during the COVID-19 outbreak: considerations for the rapid introduction of remotely supported (eHealth) pain management services. PAIN 161: 889–893. [View]
- Blyth FM (2010) The demography of chronic pain: an overview. In: Croft P, Blyth FM, van der Windt D, editors. Chronic pain epidemiology: from aetiology to public health. New York: Oxford University Press. ISBN 9780199235766.
- Blyth FM, Van Der Windt DA, Croft PR (2015) Chronic disabling pain: a significant public health problem. Am J Prev Med 49: 98–101. [View]
- Rice AS, Smith BH, Blyth FM (2016) Pain and the global burden of disease. PAIN 157: 791–6. [View]
- Choiniere MD, Dion P, Peng R, Banner P, Barton A (2010) The Canadian STOP-PAIN Project-part 1: who are the patients on the waitlists of multidisciplinary pain treatment facilities? Can J Anesth 57: 539–48. [View]
- Lynch ME, Campbell FA, Clark AJ, Dunbar MJ, Goldstein D (2008) A systematic review of the effect of waiting for treatment for chronic pain. PAIN 136: 97–116. [View]
- Stannard C (2018) Opioids for pain in Europe: differing problems and differing solutions. In: Eccleston C, Wells C, Morlion B, editors. European pain management. Oxford: Oxford University Press pp. 225–42. [View]
- Buhrman M, Gordh T, Andersson G (2016) Internet interventions for chronic pain including headache: a systematic review. InternetInterv l4: 17–34. [View]
- Comerci GJ, Katzman J, Duhigg DO (2018) Controlling the swing of the pendulum. NEJM 2018 378: 691–3. [View]
- Glod S (2017) The other victims of the opioid epidemic. N Engl J Med 376: 2101–2. [View]
- https://choir.stanford.edu/
- http://pain-out.med.uni-jena.de
- Hegarty DA. Survey of pain related telehealth papers on PubMED 2000–2020 (submitted for publication)
- Palermo TM, Slack M, Zhou C, Aaron R, Fisher E, Rodriguez S (2019) Waiting for a pediatric chronic pain clinic evaluation: a prospective study characterizing waiting times and symptom trajectories. J Pain 20: 339–47. [View]
- Dario AB, Cabral AM, Almeida L, Ferreira ML, Refshauge K, Simic M, Pappas E, Ferreira PH (2017) Effectiveness of telehealth-based interventions in the management of non-specific low back pain: a systematic review with meta-analysis. Spine J 17: 1342–51. [View]
- Martorella G, Boitor M, Berube M, Fredericks S, LeMay S, Ge ?linas C (2017) Tailored web-based interventions for pain: systematic review and meta-analysis. JIMR19: e385. [View]
- Adamse C, Dekker-Van Weering MG, van Etten-Jamaludin FS, Stuiver MM (2018) The effectiveness of exercise-based telemedicine on pain, physical activity and quality of life in the treatment of chronic pain: a systematic review. J Telemed Telecare 24: 511–26. [View]