- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Impact of the COVID-19 Pandemic on Urological Services
- Home
- Back to Journal
- Article Details
Abstract
Background: The world is currently under the grasp of the COVID-19 pandemic. Medical priorities are rapidly changing and are being enforced across all health-care systems. Urologists were obliged to minimize their clinical activity and junior urology trainees have been deployed to assist on COVID-19 wards. The repercussions on urological patient outcomes for delayed treatments and diagnosis remain to be defined.
We have reviewed the current literature including online publications and webinars, pertaining the impact of COVID-19 pandemic urology services.
Methods: The authors carried out literature search of the available databases (Medline/PubMed, EMBASE, Cochrane database, NICE guidelines and Google Scholar). The key words used were COVID-19, Corona virus, pandemic, urological services. The relevant studies were scrutinized and full text versions were retrieved. The references to all the retrieved texts were searched for further relevant studies.
Conclusion: Urologists need all the support needed with updated, timely and corrected indications for managing urological patients during the pandemic, to guide difficult decision-making. Despite the evolving management of COVID-19, the effect of the pandemic will inevitably produce negative repercussions on overall patient outcomes, but these are still unknown and impossible to quantify. Ultimately, this unparalleled health situation will assist in revealing the real necessity for the high number of aggressive diagnoses and treatments normally offered widely to (too) many patients, in a urological setting and beyond.
Keywords: COVID-19; Corona virus; pandemic; surgical services; urology; guidelines
Introduction
The rapid escalation of the COVID-19 pandemic has made a huge, rapid and lasting impact on health services worldwide. The World Health Organization (WHO) has officially expressed its deep concerns about the exponential growth in the number of reported cases, which has passed one million at the time of writing this paper. Health services had to be stopped, rescheduled, redeployed, restructured and adapted to the new situation, according to the infrastructural, financial and cultural frameworks in their respective countries. We probably will never again practice medicine in many aspects as we knew it. Priorities and resources had to be thought over, new unexpected infrastructural challenges had to be rapidly addressed on all levels, from facemasks to mammoth makeshift hospitals, and we did not even have time to think about how the backlog in medical services that this may have created will be tackled in the near and medium future.
Surgical practice has been affected in its own particular ways. Practice patterns, patient communication, triaging and prioritizing of services and operations all have changed in a big way. Elective surgeries have all but ceased in many places.
This is true for urology as well. Large organizations like the European Association of Urology (EAU) and the British Association of Urological Surgeons (BAUS) addressed the need for guidance and recommendations to help urologists to make the right choices in such unusual circumstances [1,2]. The National Health Service (NHS) in the United Kingdom has likewise addressed surgical practice under COVID-19 [3].
Without doubt, this ongoing pandemic will have its short and long term effects on the various aspects of health services. To delineate somewhat this impact, we have reviewed the recommendations and guidelines, as well as the current published evidence on the current and predicted future impact of the COVID-19 pandemic on surgical and urological hospital services.
Methods
We performed a systematic literature search of Medline/PubMed, EMBASE, Cochrane database, NICE guidelines and Google Scholar. The search terms used were COVID-19, Corona virus, pandemic, urological services. The relevant studies were screened and full text versions were retrieved. The references to all the retrieved texts were searched for further relevant studies. Two separate searches were done using a combination of terms as both, Medical Subject Headings (MeSH) and keywords.
In the following, we will address various aspects of health services in surgery in general, and urology in particular, that have been impacted by the pandemic
COVID19 Impact on Surgery
1. Impact on Surgical Services in General
The COVID-19 pandemic imposes a significant burden on national health services in general, and on surgical services in particular. Everywhere, there are limited resources for dealing with such a vast number of infected cases and a lack of sufficient intensive care infrastructure to care for the high number of seriously ill cases.
This resulted in a redeployment of healthcare workers in order to boost the numbers of available frontline healthcare professionals. Junior doctors and nurses from other specialties were made to work in emergency and intensive care units.
To minimize COVID-19 transmission, the use of Personal Protective Equipment (PPE) became a gold standard recommendation.
Surgical specialties have witnessed one of the most dramatic changes resulting in rapidly decreasing numbers of elective operations. Operating theatres, surgical HDU/ ICU beds, and recovery units have all been converted to COVID-19 intensive care beds. Respirators have become a sought-after commodity and been left on stand-by for COVID-19 cases. Anesthetists have been redeployed to care for the respirator-dependent patients. For even the most experienced surgeons, this means interpreting the meaning of “elective” and balancing this definition with the individual health risk of each patient has become a challenge [4].
2. Impact on Training
Residents in surgical specialties are essential for any national healthcare workforce. The effect of the COVID-19 pandemic on this group is becoming clear, with the main impact occurring at the early stage of the pandemic. NHS England along with all deaneries across the UK advised that trainees in non-acute areas were asked to support urgent and unplanned care, such as medical admissions and the subsequent management of those patients. That might possibly extend to providing support to clinical teams in other disciplines.
It was emphasized that trainees must not be asked to undertake any activity beyond their level of competence and are advised to seek senior workplace guidance if needed.
Redeployed trainees should be provided with appropriate induction prior to starting work and they should be reviewed weekly with updates provided to the relevant Postgraduate Dean on to ensure adequate supervision in the host environment / specialty, and that they continue to work within the limits of their competence appropriate to their stage of training.
Where learning outcomes are not achieved, these issues will be taken into consideration at the trainee’s next Annual Review of Competence Progression (ARCP) which will inform future training requirements and placement planning.
Royal Colleges are being asked for maximum flexibility to support the service to receive the doctors it needs, in the right place and at the right time. Medical Directors and Deans have been liaising with all the colleges to ensure delivering annual reviews on time, when possible. With respect to college examinations, where possible, remote access to machine marked exams is to be adopted. As the peak has passed, the trainees (in cold specialties) are slowly going back to their usual daily routine, with being on standby if/when needed [5].
An international survey was carried out among neurosurgeons around the world between March and April 2020. Most of the respondents were neurosurgeons in their early training. Four hundred and thirty-seven (88.8%) reported at least some disruption of their practice caused by the pandemic, with 52.2% saying that all elective cases and clinics have been shut down by hospital or practice policy. 302 (61.4%) neurosurgeons, thought that their elective practice ought to be shut down totally. A total of 226 respondents (46.1%) reported that their operative volume had dropped more than 50% [6]. It goes without saying, that this has an enormous impact on surgical training and skill development. All surgical specialties have experienced a similar downturn, and neurosurgeons may be just representative for those.
3. Change in Practice
Due to the highly infective nature of the COVID-19 virus, several guidance has been rapidly issued with the aim of protecting healthcare professionals and their patients. Allocating dedicated senior staff to key management roles is crucial to minimize the spread of the disease. All staff must be properly trained for donning and disposal of Personal Protection Equipment (PPE), such as face masks (level 2 or 3 Filtering Face Piece (FFP) depending on the aerosol-generating risk level), eye protection, double non-sterile gloves, gowns, suites, caps, and socks [7].
In the United Kingdom, NHS introduced several personal protective policies for hospital staff, such as no belts, wallets or cash/coins to be carried, only contactless bank cards to be used for any payments, and the use mobile phone to be restricted as much as possible. Before going home at the end of a shift, utensils such as pen and stethoscope, and hospital notes should be placed in a plastic re-sealable bag after cleaning with 70% alcohol. They should not be taken outside the hospital. Also, ‘bare below elbows’ in hospital is to be practiced vigilantly. Hands should be cleaned up to the elbows with soap and water just before leaving the ward, and no surfaces should then be touched until the healthcare worker has left the hospital’s main gate.
Routine examination of patients should be avoided if possible. A distance of 1–2 metres away from patients during ward rounds is recommended.
When getting close to patients is unavoidable, i.e. during examination, taking blood samples or any intervention, PPE (FF2 mask at least or surgical mask + full face visor, both with full sleeve apron) should be worn, and patients should be asked to turn their faces away from the examining doctor/nurse and use tissue to cover their mouths and noses even when they use a face mask.
Mobile phones, spectacles and computer keyboards should be cleaned with 70% alcohol at least once before leaving the ward and/ or the hospital [8].
4. Outpatient Clinics
Social distancing is paramount to minimize the impact of the pandemic and help providing safer healthcare. This constitutes a challenge when it comes to outpatient consultations that would normally require face-to-face consultations, clinical examinations, and exposure of the healthcare staff to patients, and of patients to each other. Hence it seems prudent to use alternative modern technologies. Virtual phone clinics and telemedicine consultations have been set up in many places. Telemedicine comes however with its own challenges. Clinicians might feel the system being less effective as it loses an important part of the communication, especially in telephone clinics as opposed to video conferencing. These clinics would be at risk of disconnection should the system be overwhelmed, and this could potentially result in a breakdown of communication and delays in the consultation. Patients must be identified prior to the clinic as to hearing difficulties. Those would then need to “attend” these virtual clinics with a relative to facilitate the online communication [9].
Some patients might still require face to face consultations. A COVID-free building or wing within the hospital complex could be set aside and be used for such clinics. Patient visits must be spaced out in order to allow through cleaning of the facility after each use. The same could be true for treatment rooms, in urology for example for catheter insertions or urgent cystoscopies [10]. In some places, private health care facilities that do not treat any elective cases at the moment, have been taken over by public health services as such COVID-free outsource facilities.
5. Impact on Operation Waiting Lists
The NHS in the UK is one example of a health care system operating traditionally with operation waiting lists. Waiting lists exist in many countries around the globe. The NHS has always been under pressure of meeting the demands of the waiting lists. Since January 2013, patient numbers on the waiting lists for routine procedures have been growing significantly at about 7.7% per year, whilst waiting times have gone up by about 6% per year in parallel. Because of a seasonal increase of hospitalizations in winter, there was an elective shutdown in January 2018 which led to an estimated loss of up to 50,000 inpatient operations in one month alone. Whilst this backlog still exists, a three-month COVID-19 enforced shutdown potentially and practically adds about 5 months’ worth of cases to that existing waiting list (possibly due to the daily increase of the individual patients waiting times currently, and the potential surge in referrals once the situation clarifies. Added to that the potential limitations of the existing resources in the presence of large number of COVID-19 infected patients in hospitals). This in light of the existing average 25-week routine waiting times which should ideally be <18 weeks as per government targets [11].
According to hospital activity statistics, inpatients stand for about 15% of all elective attendances. A three-month shutdown might mean a loss of 150.000 elective operations in the UK alone [12].
Patient’s Management in Operating Theatres
Both laminar flow and conventionally ventilated theatres should remain fully on during surgical procedures where patients may have COVID-19 infection. Air can bypass filtration through a poorly fitted respirator.
Staffs closest to aerosol generation procedures are most at risk. The rapid dilution of these aerosols by theatre ventilation system will protect operating room staff. Air exiting operating theatres to nearby areas will be highly diluted and is not considered to be a risk. COVID-19 positive case should be communicated to theatres prior to patient transfer to theatres.
The patient should be directly transferred to the operating theatre and should wear a surgical mask if possible.
Anesthesia and recovery should both occur in the theatre with minimum staff present. Staff should wear protective clothing but only those within 2 meters of an aerosol generating procedure, such as performing intubation; need to wear FFP3 respirators, disposable fluid repellent coveralls or long sleeved gowns, gloves and eye protection. Instruments and devices should be decontaminated in the normal manner in accordance with manufacturers’ advice. The theatre should be cleaned as per local policy for infected cases, with special attention to contact areas on the anesthetic machine. Possible or confirmed cases of COVID-19 should be placed at the end of the list where feasible. After the patient leaves the theatre, 5 minutes should pass before staff without respirators can enter and clean [13].
6. Impact on Elective Surgeries
The COVID-19 virus was detected in the peritoneal cavity of a 78 year old man presenting with acute abdomen. It seems therefore prudent to deal with any surgical cases with extra caution [14].
Hospitals in the UK, as in most countries, have been advised to hold all non-urgent elective surgeries for at least three months in order to assist health services in coping with the COVID-19 pandemic. Hospitals were advised to discharge all inpatients that are deemed medically fit to leave. In addition, the NHS has secured capacities in independent private hospitals to expand critical care capacity to the maximum possibly needed [15].
This decision was supported by the Royal College of Surgeons in England (RCS England). They also advised that hospitals and surgeons should carefully review all scheduled elective procedures with a plan to “minimize, postpone or cancel scheduled operations, endoscopies and other invasive procedures as necessary, and shift inpatient diagnostic and surgical procedures to outpatient settings, when feasible”.
Consequently, this will lead to an increase of waiting list numbers as described above, and might overwhelm the available resources to deal with it once the crisis has settled. As a possible remedial approach, RCS England has suggested that elective surgeries could be provided on a networked basis via an interconnected system of service providers rather than in individual hospitals and clinics. This would allow for collaborative working (assisted by contractual agreements where required), flexible movement of clinical staff, and robust patient transfer arrangements according to clinical needs. This will however require senior clinical and managerial endorsement, robust contractual arrangements, and agreed coordinated protocols of care [16].
7. Prioritization Guidelines
7.1 NHS
The National Health Service (NHS) in the UK issued prioritization guidance for patients needing surgery. This guidance describes levels of surgical priority. NHS states that these new time intervals may vary from usual practice and may possibly result in a greater risk of adverse outcomes due to progression or worsening of the underlying medical condition. On the other hand, the NHS emphasized the importance to work within the resources available locally and nationally during the crisis.
Patients requiring surgery during the COVID-19 pandemic have been classified as follows:
- Priority level 1a: Emergency - operation needed within 24 hours
- Priority level 1b: Urgent - operation needed with 72 hours
- Priority level 2: Surgery that can be deferred for up to 4 weeks
- Priority level 3: Surgery that can be delayed for up to 3 months
- Priority level 4: Surgery that can be delayed for more than 3 months
Urological procedures have been classified using these levels (Table 1). The NHS classification seems to be complementary to the BAUS classification addressed below [17].
Table 1: NHS classification of urological procedures according the the NHD-defined priorities.
|
Priority 1a Emergency (24hrs)
|
Renal obstruction with infection – not responding to conservative Rx Renal/ureteric trauma requiring open surgery Bladder trauma requiring open surgery Genital trauma/amputation/priapism (24hrs) Fournier’s gangrene Haematuria/uncontrolled haemorrhage – causing haemodynamic instability and unresponsive to conservative Rx Acute urinary retention (with/without renal impairment) Peno-scrotal abscess |
|
Priority 1b Urgent (up to 72 hrs)
|
Upper urinary tract obstruction Renal stones – pain/ impairment not responsive to conservative Rx Penile fracture |
|
Priority 2 Up to 1 month
|
MDT directed testicular cancer surgery – non- metastatic. MDT directed penile cancer surgery including inguinal node surgery. MDT directed bladder cancer surgery – invading bladder muscle. MDT Directed renal cancer surgery – not bleeding. MDT directed upper tract transitional cell cancer surgery MDT directed bladder Cancer surgery -high risk carcinoma-in- situ. MDT directed inguinoscrotal sarcoma surgery Acute Urinary Retention (definitive management) – Bladder neck stenosis post RARP. |
|
Priority 3 Up to 3 months
|
MDT directed prostate cancer surgery – high/ intermediate risk Stent removal/ exchange Haematuria – investigation for non-visible MDT directed bladder cancer surgery (not invading muscle) MDT Directed penile cancer surgery (low grade and premalignant). |
|
Priority 4ver 3 months
|
Female urology for benign conditions (eg incontinence/ prolapse/Sacral Nerve Stimulator/ fistula/urethral diverticulum/ Andrology/GU Surgery (surgery for erectile dysfunction/ male fertility surgery/ urethral stricture/ gender reassignment. Endourology – uncomplicated stones/ percutaneous nephrolithotomy/ pelviureteric obstruction MDT directed prostate cancer surgery (low risk) MDT directed bladder cancer surgery – superficial transitional cell cancer Uncomplicated Uncomplicated small/intermediate testicular lesions Bladder outflow surgery Benign penoscrotal surgery |
7.2 EAU
The EAU has issued an outstanding set of guidelines, considering the gravity of the situation and the diversity of different healthcare systems in European countries.
Patients are categorized according to the severity of their clinical condition:
- LOW PRIORITY: Clinical harm (progression, metastasis, loss of function) very unlikely if postponed for up to 6 months.
- INTERMEDIATE PRIORITY: cancel but reconsider in case of increase in capacity; not recommended to postpone for more than 3 months: Clinical harm (progression, metastasis, loss of organ function) possible if postponed 3 months but unlikely.
- HIGH PRIORITY: prevent any delay over 6 weeks. Clinical harm (progression, metastasis, loss of organ function and death very likely if postponed > 6 weeks).
- EMERGENCY: cannot be postponed for more than 24 hours. “Loss of life or limb” condition.
The high virulence of the COVID virus, along with the necessary social confinement and isolation, has led to further emerging recommendations; EAU advised for testing staff and patients for COVID, if resources are available, and according to local guidelines. Since surgery is harmful with a high mortality risk in COVID-19 positive patients, surgery is to be postponed if at all possible and it should be only offered for high-priority and emergency cases [18].
Intermediate priority patients can be treated if capacity becomes available, but not during the COVID surge. In addition, older patients with comorbidity are at severe risk of COVID infection with fatal outcome. Therefore, their surgeries must be carefully considered and only go ahead in high-priority cases when surgery is the only alternative.
EAU advised to follow the local recommendations for personal protective equipment (PPE), if resources are available. But also EAU stressed on the use of full PPE when dealing with COVID positive patients according to the World Health Organization (WHO). This should include double gloves, gowns, face shields and virus-proof masks.
Ideally, intubation and extubation should preferably take place in a negative pressure room if available. In addition, non-essential staff should stay outside the operating room during the procedure. During surgery, the electro surgery units should be set to the lowest possible settings to reach the required effect, and if possible, EAU recommended reducing the use of monopolar electrosurgery, ultrasonic dissectors, and advanced bipolar devices as these can lead to particle aerosolisation. If monopolar diathermy is to be used, handheld devices with attached smoke evacuators should be utilized. Finally, surgical equipment of COVID positive or suspected patients are to be cleaned separately [19].
7.3 BAUS
Due to the high demand for intensive care unit capabilities to support COVID-19 patients, BAUS has issued a scheme for classifying urological procedures based on their clinical priorities (Table 2).
Table 2: BAUS prioritisation of urological procedures.
|
Top priority |
Less priority |
Least priority (first to be cancelled) |
|
Testicular torsion |
Cystectomy (low risk) |
Day surgery, egvaricocele/ hydrocele |
|
Obstructed infected kidney |
TURBT (low risk) |
Benign nephrectomy |
|
Abscess / Gangrene |
Radical prostatectomy |
Andrology |
|
Cystectomy (high risk) |
Nephroureterectomy (low risk ) |
Functional/ reconstructive surgery |
|
TURBT (high risk) |
|
Percutaneous nephrolithotomy |
|
Radical nephrectomy (T2+) |
|
TURP,HOLEP, and other procedures for benign prostatic enlargement |
|
Nephroureterectomy (high risk ) |
|
|
|
Inguinal orchidectomy(testis cancer) |
|
|
|
Ureteroscopy with ureteric stone / stented patient |
|
|
8. COVID-19 Positive Urological Patients
The EAU recommended that a COVID-dedicated Operating Room (OR) should be prepared. For endourological procedures, a mobile C-arm-based fluoroscopic X-ray system and experienced personnel for its handling should be in this special OR. The whole operating team must don appropriate and complete PPE.
All minimally invasive procedures should be performed by experienced surgeons and with the minimum number of experienced OR staff members present. No external observers are allowed.
A closed system should be used during endoscopic procedures including the evacuation of irrigation fluid.
8.1 Laparoscopic and Robotic Surgery
No evidence exists yet regarding an aerosol presence of the COVID-19 virus released during minimally invasive abdominal surgery [20].
When conducting a laparoscopic procedure, smoke evacuation systems with active filtered smoke evacuation mode, capable of filtering aerosolized particles from the carbon dioxide should be applied.
Special care must be taken when introducing instruments through the laparoscopic trocars. During insertion of the instrument, there is a definite risk of aerosolized particles escaping from the intra-abdominal cavity. Inserting 8 or 5 mm instruments in a 12 mm da Vinci trocar without a reducer should not be practiced. Turning off and venting the gas through a filter prior to specimen extraction is recommended. Consultation with the CO insufflation manufacturer may be necessary to ensure proper settings are selected for maximal filtration effect.
For (robot-assisted) laparoscopy and retroperitoneoscopy, the lowest allowed intraabdominal pressure with the use of intelligent integrated insufflation systems is recommended [20].
Electrocautery power should be used sparingly, with the setting reduced as much as possible in order to decrease the surgical smoke production especially in laparoscopic surgery. During access, electrocautery should be provided with an automatic suction system [19].
9. Disease Specific Recommendations
For the UK, BAUS made significant changes to the national guidelines for suspected urological cancer cases in the light of the current pandemic. In the USA, the American Urological Association (AUA) likewise issued amended guidelines. In the following, both will be outlined.
9.1 Prostate Cancer
9.1.1 Suspected Prostate Cancer
For suspected Prostate Cancer (PCa), BAUS recommends continuing with current diagnostic and treatment protocols as long as practically and safely possible, but has warned that the diagnostic and treatment pathways may not be sustainable.
BAUS also advised on the potential significant reduction in radiological investigations (US/CT/MRI) since radiology staff are likely to be deployed to emergency services.
MRI scanners could be a potential source of COVID-19 transmission due to their enclosed space resulting in a reduced access/availability for cancer patients. CT scanners are likely to be vital resources for the respiratory/ITU teams.
Despite the availability of PSA blood testing, it would not be safe for elderly/frail patients to attend for blood testing at present.
COVID recommendation policy is to avoid TRUS prostate biopsy if possible due to risk of sepsis which will need hospital admission and possible critical care support [21].
In Men with PSA < 20 ng/ml, US estimation of prostate volume is recommended. If PSA density >0.15, patients will be offered prostate biopsy as an NHS priority 3 (within three months). If PSA density < 0.15, then patients will have a repeat PSA in 6 months. Men with PSA >20 ng/ml are offered a biopsy as an NHS priority 2 (within 4 weeks).
In the USA, the American Urological Association (AUA) similarly recommended prostatic biopsy (preferably transperineal biopsy, to minimize infectious risks and fecal exposure) for those at a high risk of having prostate cancer, including prostate specific antigen (PSA) greater than 20, rapid PSA doubling time less than 6 months, digital rectal examination concerning for clinical T3 disease, and/or they have local or systemic symptoms of the disease.
However, unlike BAUS, AUA advised carrying out MRI initially; delay biopsy up to 3 months if possible, as such a delay in diagnosis of high risk prostate cancer by according to AUA is unlikely to change long-term oncologic outcome.
9.1.2 Established prostate cancer
As per BAUS, men with low/intermediate risk non-metastatic PCa will be offered active surveillance, with a repeat PSA in 6 months or Bicalutamide 50mg OD.
In patients with high risk non-metastatic PCa, BAUS recommends LHRH or Bicalutamide 150mg OD until curative therapy is again available in the form of radical prostatectomy or radiotherapy.
In men with metastatic prostate cancer, BAUS recommends LHRA analogues. Primary chemotherapy is to be deferred [21].
For patients on primary Androgen Deprivation Therapy (ADT), PSA follow-up can be stretched to 6 monthly.
Radiotherapy should be avoided altogether due to its potential risk of COVID-19 transmission in enclosed spaces. Urgent cases can be an exception, such as rapid loss of function e.g. spinal cord compression.
The BAUS panel acknowledges that this will be exposing an increasing proportion of men to hormone therapy who would not ordinarily have chosen this modality [21].
In the USA, National Comprehensive Cancer Network (NCCN) together with AUA concur with BAUS in avoiding staging, active surveillance, confirmatory testing/monitoring, and treatment of patients with very low, low, and favorable Intermediate Risk (IR), until deemed safe.
AUA also advised against prophylactic whole pelvic radiation therapy during this time due to the increased risk of grade IV lymphopenia. Also, for patients with non-metastatic disease, NCCN/AUA recommended avoiding initiating Androgen Deprivation Therapy (ADT) for patients with a Prostate-Specific Antigen (PSA) doubling time of >9 months.
For patients with asymptomatic Unfavorable Intermediate Risk (UIR), high risk, and very high risk (HR) prostate cancer can defer further staging and radical treatment until deemed safe.
Neoadjuvant ADT (preferably 3, 4 or 6-month formulations rather than 1-month injections) should be considered in asymptomatic UIR and HR patients planning to receive definitive radiation therapy (RT). This may safely be given for up to 4–6 months as necessary.
AUA/NCCN advised deferring the initial post-treatment assessment until deemed safe. Alternatively, telehealth visits with discussions of PSA and testosterone could be considered.
If it is deemed safe for patients to receive RT, the shortest safe external beam RT (EBRT) regimen should be used. This can consist of 5 to 7 fractions, consistent with current NCCN Guidelines.
For patients with advanced disease, NCCN recommended non-myelosuppressive regimens when alternatives exist to minimize risk of immunosuppression and infectious complications.
When cytotoxics are used NCCN advised growth factor support with administration of same-day growth factor injections or pegfilgrastim to minimize visits. Consider deferring sipuleucel-T until COVID-19 risk has resolved given risks of exposure in Red Cross centers and hospital infusion centers [22].
In a retrospective review of 128,000 men with intermediate and high-risk prostate cancer (PC) underdoing radical prostatectomy (RP) from 2010–2016, with immediate RP bing defined as RP within 3-months of diagnosis, while delayed RP was analyzed in 3-month intervals up to 12-months, Ginsburg et al. did not find a significant difference in odds of adverse pathology, upgrading, node positive disease, or post-RP secondary treatments between the two groups. AUA recommended delay in RP, balancing care in the current pandemic [23].
10. Haematuria
BAUS guidance on haematuria patients was adopted from the IDENTIFY study; a prospective international multi-centre observational cohort study that showed the overall prevalence of urological malignancy was 12.2% (10.4% bladder, 0.6% ureteric/ renal TCC, 1.2% renal); which was 16.4% of the VH group and 5.0% of the NVH group. 85% of malignancies presented with VH).The authors provided BAUS with an update on their study during COVID-19 (Figure 1) [24].
Patients with a newly diagnosed bladder tumor will be offered transurethral resection of bladder tumor (TURBT) only in cases of solid and/ or actively bleeding tumors. Re-TURBT will only be offered to very high risk cases of Non-Muscle Invasive Bladder Cancer (NMIBC) with clinical suspicion of under-staging [21].
The AUA has issued guidelines that largely concur with BAUS (Table 3).
Table 3: AUA recommendations for hematuria and bladder cancer patients.
|
Procedure |
Indication |
recommendation |
Comments |
|
Diagnostic cystoscopy |
Gross hematuria Microscopic hematuria with risk factors (smoking history, occupational/ chemical exposure, irritative voiding symptoms). Microscopic hematuria without risk factors |
Consider performing full evaluation without delay. Consider delaying evaluation up to 3 months unless patient is symptomatic. Consider delaying evaluation up to 3 months unless patient is symptomatic |
Diagnostic yield in finding bladder cancer or upper tract malignancy is high in this group. Diagnostic yield for urinary tract malignancy is increased in this setting compared to asymptomatic patients, especially when multiple risk factors are present |
|
Surveillance cystoscopy |
Assessment of response to treatment or surveillance of high risk nonmuscle invasive bladder cancer (NMIBC) within 6 months of initial diagnosis Assessment of response to treatment or surveillance of high risk NMIBC beyond 6 months of initial diagnosis Assessment of response to treatment or surveillance of low/intermediate risk NMIBC regardless of when diagnosis was made |
Consider performing evaluation without delay Consider delaying evaluation up to 3 months Delay evaluation for 3–6 months |
There is a high risk of recurrence and/or progression within the first 6 months of diagnosis High risk patients with stable disease may be at lower risk for relapse Tumor recurrence in this group is low |
|
Induction intravesical bacillus-CalmetteGuerin (BCG) chemotherapy |
High risk or intermediate NMIBC High risk NMIBC Intermediate risk NMIBC |
These patients should be prioritized for treatment, though they may also require a delay in therapy depending on local needs/resources Stop maintenance therapy and re- evaluate its use/need in 3 months Delay indefinitely |
Induction intravesical therapy provides a significant benefit by reducing disease recurrence and progression While maintenance therapy is important, the most significant benefit from intravesical treatment is likely during the induction course |
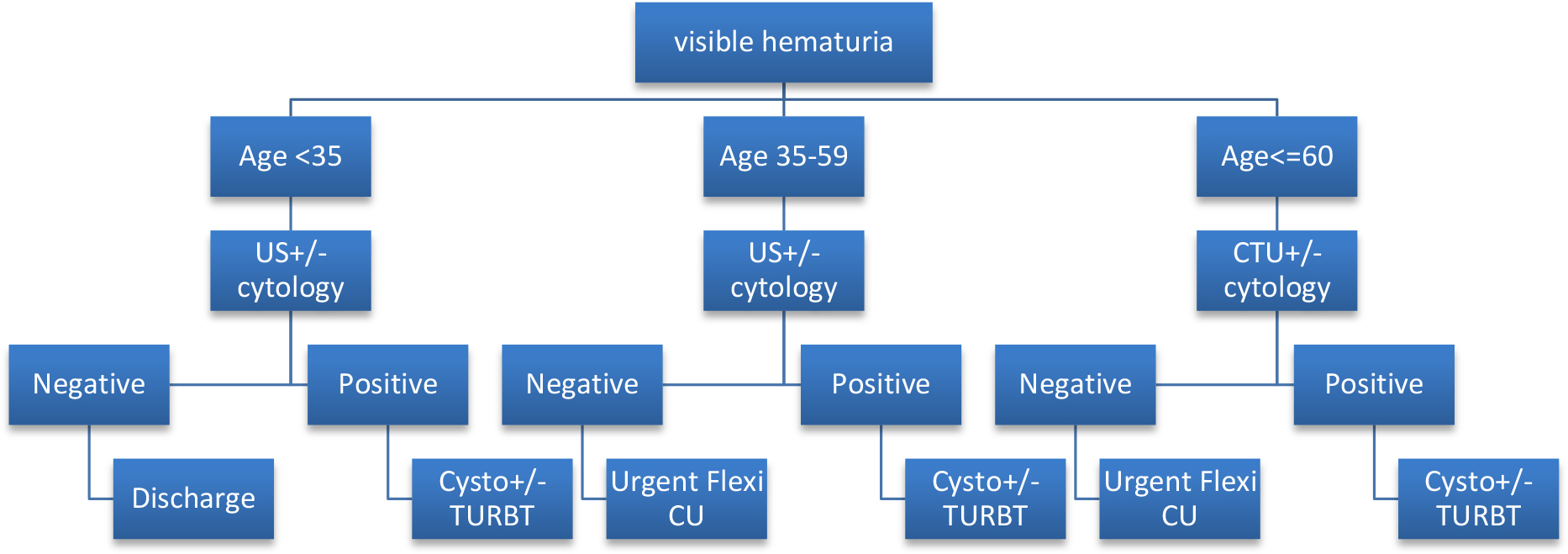
Figure 1: Diagnostic pathway for haematuria patients during COVID: recommendations from IDENTIFY study.
Patients diagnosed with small papillary tumors are offered active surveillance unless symptomatic.
Those with large papillary or solid tumors are offered primary TURBT, with the possibility for induction and maintenance of intra-vesical BCG if proven high grade [25].
11. Bladder cancer
11.1 Non-muscle invasive bladder cancer (NMIBC)
For patients with a low risk NMIBC, BAUS recommends the first follow-up flexible cystoscopy at 12 months, with a potential discharge afterwards in the absence of any recurrence.
For patients with an intermediate risk NMIBC, the first follow-up flexible cystoscopy is to be offered at 6 months, then again at 12 months. There is no consensus as yet regarding subsequent follow-up for such cases in the absence of tumor recurrence.
Patients with a high risk NMIBT, follow-up flexible cystoscopies are to be offered at 3, 6 and 12 months, respectively. Again, there is no consensus as yet regarding subsequent follow-up if there is no tumor recurrence.
BAUS advises against intra-vesical BCG or chemotherapy for NMIBC cancer due to potential immunosuppressive effects. Those already on BCG treatment should complete induction if possible, then defer further treatment [26].
According to AUA recommendations, low risk and “low grade” intermediate risk NMIBC are offered active surveillance unless symptomatic.
High grade intermediate risk and high risk NMIBC are offered primary TURBT, with induction and maintenance of intravesical BCG [26].
11.2 Muscle invasive non-metastatic bladder cancer (MIBC T2-4 N0 M0)
BAUS advises against neo-adjuvant chemotherapy (NAC). As the OR environment is considered as high risk for spreading the virus, BAUS recommends radiotherapy (RT) as first line therapy. If RT is contraindicated, a primary radical cystectomy (RC) and urinary diversion is recommended. The maximum allowed treatment delay remains at 90 days [21].
According to the AUA, MIBC patients fit for surgery are scrutinized according to the risk factors of their bladder cancer (absence of cancer variants and other adverse factors) and the availability of the local resources, bearing in mind that COVID-19 patients must be a priority for intensive care units.
Those with low risk, in the absence of sufficient resources, are offered either NAC followed by RC (hoping for improvement of the COVID situation by the time of the RC), or to be considered for a multimodality bladder preserving approach (TURBT, chemo- and radiotherapy). Also, a consideration is given to those who wish to be included in the currently available clinical trials in the USA for patients with NMIBC and MIBC that may be affected by COVID-19 AUA also acknowledges the concerns in offering NAC to patients resulting in a potential lowering of their immunity and rendering them more susceptible to COVID-19 infection [27].
12. Renal cancer
Wherever possible, patients with suspected or proven renal cancer should be managed according to currently accepted investigative and treatment strategies, until such time that resources become so limited that severe risk stratification is required. For T1a suspected and proved kidney cancers, active surveillance with imaging follow-up at 6 and 9 months is recommended.
Initially, BAUS recommended against partial nephrectomy, percutaneous ablation or stereotactic radiotherapy in the management of T1 patients during the COVID-19 pandemic. However, as the situation is evolving, and in an effort to continuously actualize recommendations, BAUS along with the NHS is recommending nephron sparing surgery, percutaneous ablation, and renal biopsy as an NHS priority 3 (within three months), always considering the availability of the local/regional resources [28].
For T1b kidney cancers, active surveillance with imaging follow-up at 3 and 6 months is recommended. Urgent nephrectomy is recommended for T2 tumors, and the highest priority for nephrectomy is given for those with T3 tumors. For metastatic renal cancer, no biopsy or cytoreductive nephrectomy is indicated. Rather, patients should be referred to the oncology department under the assumption that the role of Tyrosine Kinase Inhibitors (TKIs) would be limited during the COVID-19 pandemic [21].
13. Testicular cancer
Men presenting with a testicular mass will ideally have an ultrasound, tumor markers and a staging CT. However, BAUS acknowledges the potentially limited access to those facilities. Inguinal orchidectomy is recommended for those with testicular cancer, when access to theatres is available. BAUS recommends against insertion of testicular prosthesis.
In men with a high risk pure seminoma, active surveillance or adjuvant carboplatin is recommended as long as patients understand the need to self-isolate.
In men with a high risk non-seminoma, a single cycle of Bleomycin, Etoposide and Cis-platimun (BEP) should be administered, provided they understand the need to self-isolate [21].
Retroperitoneal lymphnode dissection (RPLND) is considered as an NHS priority 2 (within 4 weeks) for salvage procedures, and priority 3 (within 3 months) as primary procedures.
14. Urolithiasis
The COVID-19 pandemic has led to significant changes in the practice patterns of endourologists for the management of urinary stone disease.
An online survey was circulated primarily to endourologists who had contributed to the literature. Of 98 experts approached, 60 (61.2%) responded [25]. Of those, 55% and 40% changed their elective surgical treatment approach after COVID-19 by a rate of 90–100% and 75–89%, respectively. Only 5% continued as before the pandemic.
Chest CT was routinely requested 24?h before surgery by 28%, whereas now 62% requested a chest CT in case of COVID-19 suspicion. The majority of endourologists prefer regional anesthesia during the COVID-19 pandemic, depending on their hospital infrastructure. More notably, one third prefer a conservative approach for stones <2?cm and 2–3?cm in size until the pandemic settles. In addition, approximately two-thirds stated that they would postpone any auxiliary procedure because of the COVID-19 pandemic, and 51% stated that they would discharge patients on the same day or within 24?h postoperatively.
Generally, a conservative approach in managing cases of renal colic is recommended to avoid in-patient admissions. This includes telephone consultation to screen patients for history and / or symptoms suggestive of COVID-19. Any patient with suspected or confirmed COVID-19, requiring urgent endo-urological intervention, would be managed in a dedicated operating room as described above.
As per EAU, managing urinary tract stones depends on stone size and location, obstructive uropathy, symptom control, presence of indwelling ureteric stent or nephrostomy tube, and other related factors such as solitary kidney or impaired renal function (Figure 2). The general principle is conservative treatment, minimal intervention, and safe management of patients with urolithiasis. The mainstay of surgical treatment, if required by the presence of an impaired renal function, symptomatic hydronephrosis that is not responding to conservative measures and infected hydronephrosis that is not responding to medical treatment, is providing drainage of the urinary system with either a JJ stent or percutaneous nephrostomy tube until the situation settles [29].
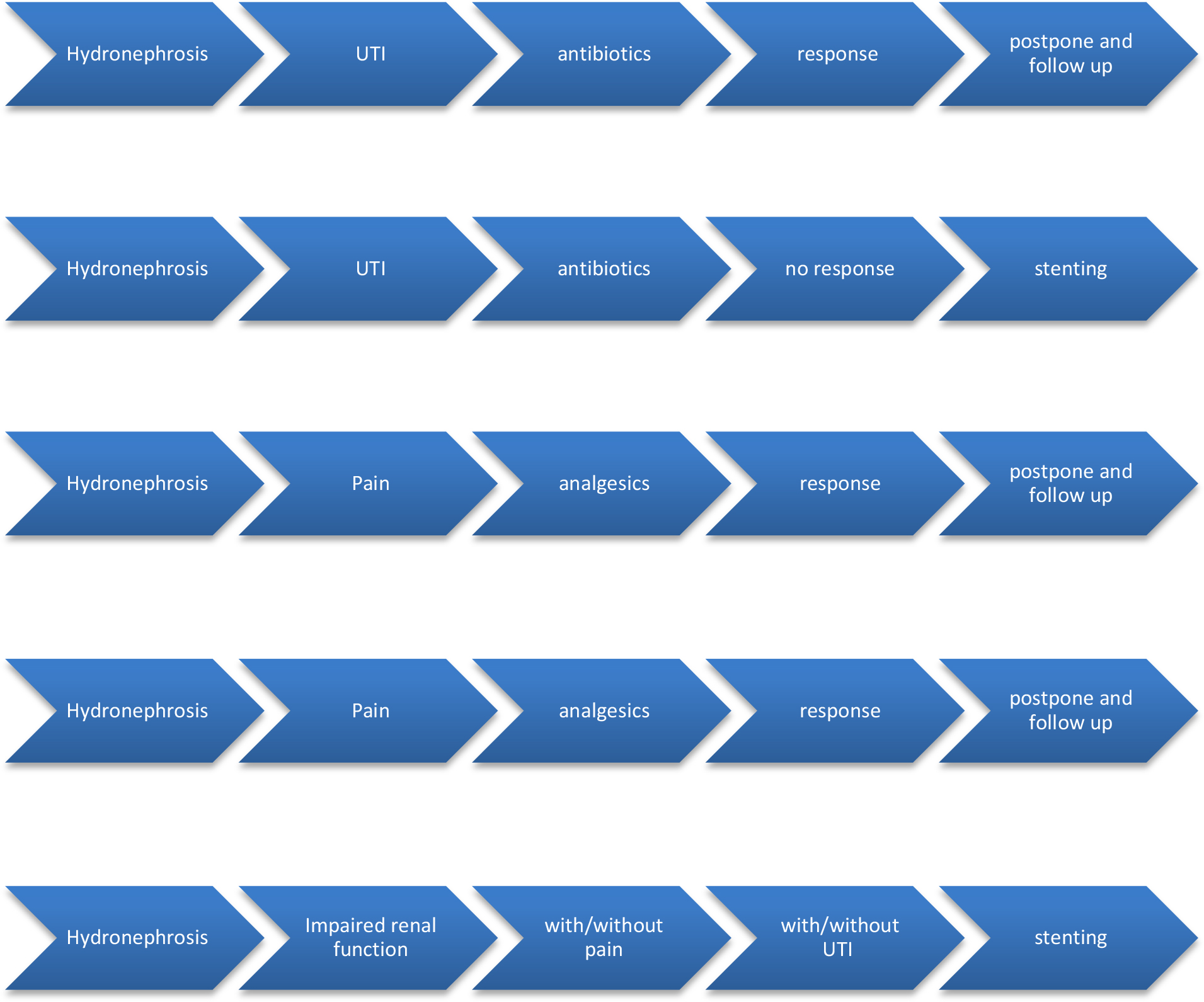
Figure 2: Management of Urolithiasisaccording to European Urology COVID-19 guidelines.
BAUS issued with a more comprehensive guidance on prioritization of patients with urolithiasis, as per NHS priorities, explained below:
Priority 1a (emergency within 24 hours)
Ureteric stones:
- Ureteroscopy (URS) for stone failing to pass with observation or ESWL.
- Prior URS with stent (risk of UTI if untreated within 4 weeks)
- URS +/- stenting for impaired renal function
- High lithogenic risk stent change
- Overdue stent change
Kidney stones:
- URS or PCNL for kidney stones with complications (sepsis, renal impairment) and upper tract Transitional Cell carcinoma (TCC)
- URS for upper tract TCC
Intermediate and low Priority (within 3 months/after 3 months respectively):
- URS/PCNL for symptomatic renal stones
- URS for asymptomatic ureteric stones
- Scheduled stent change
- Cystolitholapaxy for symptomatic bladder stones [28].
15. Andrology and Endo-urology
BAUS together with NHS England issued guidance for andrology and endo-urology procedures for the lower urinary tract, according to the NHS priorities:
Priority 1a (emergency within 24 hours):
- Genital trauma/amputation/priapism (24hrs)
- Fournier’s gangrene
- Acute urinary retention (with/without renal impairment)
- Peno-scrotal abscess
Priority 1b (within 72 hours):
- Penile fracture
- Infected prosthesis – penile/testicular/ stent
Priority 2 (within 4 weeks):
- MDT directed inguino-scrotal sarcoma surgery
- MDT directed penile cancer surgery (high grade/stage)
- Acute Urinary Retention (definitive management) - Bladder neck stenosis post RARP.
- Delayed penile implant post prolonged ischaemic priapism.
- Skin graft reconstruction post Fournier’s gangrene.
- Urgent surgical sperm retrieval (prior chemotherapy for oncology patients)
- Painful eroded penile implant (not infected)
Priority 3 (within 3 months):
- MDT Directed penile cancer surgery (low grade and premalignant).
- Painful severe phimosis
- Urethral stricture (patients with suprapubic catheter)
- Stricture with severe voiding symptoms (Qmax<5mls/recurrent UTI)
Priority 4 (more than 3 months):
- Conditions not affecting quality of life, but are time sensitive:
- Early signs of penile implant erosion.
- Stricture with flow rate of <10ml/s
- Surgical sperm retrieval (SSR) in the presence of low ovarian reserve
- Conditions not affecting quality of life, but are NOT time sensitive:
- Mild phimosis
- Hydrocele/routine scrotal surgery
- Peyronie’s disease with functional impact
- Penile implant surgery
- SSR with normal ovarian reserve (Partner) [28].
16. Female urology
Diagnostic procedures such as urodynamics should be avoided unless absolutely necessary. There are very few cases that would count as priority 2 (within 3 months):
- Suprapubic catheter (SPC) insertion when the risk of long term catheterization exists.
- Open/endoscopic removal of bladder stone in a symptomatic neuropathic patient.
- Vesico-vaginal fistula repair.
- Removal of eroded device/implant.
- Excision of symptomatic urethral diverticulum.
- Botulinum toxin injection in neuropathic high pressure bladders [28].
17. Pathology specimens:
Ideally, the COVID-19 status of patients from whom pathological specimens are taken should be known and reported to the pathology department. In its absence and if a fresh-frozen specimen is absolutely necessary, the amended protection principles should be applied for technical and medical staff. The virus can survive temperatures of –20?°C, the temperature used for cutting of fresh-frozen sections. The virus remains on surfaces such as glass, metal, and plastic for up to 9 days, but can be inactivated by surface disinfection with ethanol (62–70%), hydrogen peroxide 0.5%, or sodium hypochlorite 0.1% within 1?minute.
Therefore, it is extremely important to reduce fresh-frozen sections on a strict necessity basis, as cryostat disinfection takes a long time and many laboratories have only one cryostat available for fresh-frozen sections. Formalin significantly decreases the infectivity of the virus on day 1, and a temperature of 56?°C for 90?min, 67?°C for 60?min, or 75?°C for 30?min seem to render the virus non-infectious. Paraffin for inclusion is mostly used at a temperature of 60–65?°C for 120?min, so fixed and embedded tissue sections are most likely to be safe [30].
18. Post-operative follow up
Following discharge of surgical patients, in order to minimize the risk of transmission, tele-medicine is recommended. Remote consultations and virtual multidisciplinary team meetings (MDT) should be set up to recommend the best available treatment to an individual patient.
If patients need to be assessed physically, potential or proven COVID-19-positive patients must be treated according to local, national and WHO-requirements. In that case, a comprehensive and robust infection control system should be followed.
As the waiting lists are likely to suffer from delayed cases, and to overcome this in the most efficient way, networks of expert high-volume centers at a regional, national or even international level could guarantee the continuity of oncological care in an appropriate way, ensuring the availability of in-patient beds and the timely management of the new patients.
For oncology patients requiring neo-adjuvent/adjuvant chemotherapy, testing for COVID-19 should be considered before any high-dose chemotherapy. Lastly, patients are encouraged to take full advantage of digital self-service applications to avoid contact with others to reduce the risk of cross infections [31].
19. Restarting elective surgical procedures
Elective operations might be feasible as resources become again available. The RCS England introduced a checklist with some of the main criteria that should be taken into account in the initial stages of resuming planned surgery (Table 4) [32].
Table 4: RCS England Elective Surgery Checklist Criteria.
|
Criteria for the recovery of planned surgical activity |
Yes/no |
Action |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Conclusion
The COVID-19 pandemic is unlike anything seen before in the modern world. The current pandemic emphasizes the significance of a sensible utilization of financial and human resources. Conserving assets and manpower is of utmost importance in healthcare. It is essential to protect the urologists to carry out their tasks through the pandemic. A sensible effort should be made to reduce the risk of infection in this sector. A high mortality rate within this group would be detrimental.
Authors’ Contribution
N Buchholz: Data Collection, Manuscript writing and editing.
A Al Samarraee: Project development, Manuscript editing.
A Thwaini: Project development, Manuscript writing
References
- Ribal M, Cornford P, Briganti A, Knoll T, Gravas S, et al. (2020) European Association of Urology Guidelines Office Rapid Reaction Group: An Organisation-wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. European Association of Urology 78: 21–28 [View]
- https://www.baus.org.uk/about/coronavirus_covid-19.aspx
- http://https//www.nhs.uk/conditions/coronavirus-covid-19/
- Adrian Diaz (2020) Elective surgery in the time of COVID-19. Am J Surg 219: 900–902. [View]
- https://www.hee.nhs.uk/coronavirus-information-trainees
- Jean W, Ironside N, Sack K, Felbaum D, Sayed H (2020) The impact of COVID-19 on neurosurgeons and the strategy for triaging non-emergent operations: a global neurosurgery study. ActaNeurochir (Wien) 162: 1229–1240. [View]
- Coccolini F, Perrone G, Chiarugi M, Di Marzo F, Ansaloni L, et al. (2020) Surgery in COVID-19 patients: operational directives. World J Emerg Surg 15: 25. [View]
- Sellwood C (2017) Operating Framework for Managing the Response to Pandemic Influenza. NHS England team. [View]
- Anthony S, Emma T, Centaine S et al. (2019) Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). Journal of telemedicine and telecare. 26: 309–313. [View]
- Gareth Iacobucci (2020) Covid-19: all non-urgent elective surgery is suspended for at least three months in England. Thebmj 368: m1106. [View]
- https://www.theguardian.com/society/2020/may/14/a-and-e-attendance-england-record-low-covid-19-lockdown
- https://elsjbsprodcdn.jbs.elsevierhealth.com/pb/assets/raw/Health%20Advance/journals/eururo/EURUROL-D-20-00649-1587127530920.pdf
- https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/886668/COVID19_Infection_prevention_and_control_guidance_complete.pdf.
- Coccolini F, Tartaglia D, Puglisi A, Giordano C, Pistello M, Lodato M, Chiarugi M (2020) SARS-CoV-2 Is Present in Peritoneal Fluid in COVID-19 Patients. Ann Surg 272: 240–242. [View]
- https://www.rcseng.ac.uk/standards-and-research/standards-and-guidance/good-practice-guides/coronavirus/covid-19-good-practice-for-surgeons-and-surgical-teams/
- https://www.hsj.co.uk/emergency-care/how-covid19-may-impact-nhs-elective-waiting-times/7027123.article
- https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/C0221-specialty-guide-surgical-prioritisation-v1.pdf.
- Lei S, Jiang F, Su W, Chen C, Chen J, et al. (2020) Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. The Lancet 21: 100331 [View]
- https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=6&cad=rja&uact=8&ved=2ahUKEwjrvub86ILpAhUuA2MBHSBYDj0QFjAFegQIAxAB&url=https%3A.
- https://uroweb.org/eau-robotic-urology-section-erus-guidelines-during-covid-19-emergency/
- www.BAUS.org.uk
- https://www.nccn.org/covid-19/pdf/NCCN_PCa_COVID_guidelines.pdf
- Kevin B. Ginsburg K., Curtis G., Timar R., George A., Michael L. Cher M. (2020) Delayed Radical Prostatectomy is Not Associated with Adverse Oncological Outcomes: Implications for Men Experiencing Surgical Delay Due to the COVID-19 Pandemic. JUrol 204: 720–725. [View]
- Khadhouri S, Gallagher K, MacKenzie K, Shah T, Gao C, Moore S (2020) IDENTIFY:The investigation and detection of urological neoplasia in patients referred with suspected urinary tract cancer: A multicentre cohort study. Int J SurgProtoc 21: 8–12. [View]
- Katz E, Stensland K, Mandeville J, MacLachlan L, Moinzadeh A, et al (2020) Triaging Office-Based UrologY Procedures During the COVID-19 Pandemic. Jurology 204: 9–10. [View]
- Silvia B, Franco G, Guido G (2020) Endourological Stone Management in the Era of the COVID-19. Euro Urol 78: 131–133. [View]
- Carvalho, Filipe LF, Galloway, LanAnh S, Saoud, (2020) Considerations about Non-Metastatic Bladder Cancer Management during the COVID-19 Pandemic. Bladder Cancer 6: 99–106. [View]
- https://www.rcsed.ac.uk/professional-support-development-resources/learning-resources/webinars/covid-19/urology-in-the-covid-19-era-how-do-we-transition-to-the-new-normal
- Tefik T, Guven S, Villa L, Gokce M, Kallidonis P, et al. (2020) Urolithiasis Practice Patterns Following the COVID-19 Pandemic: Overview from the EULIS Collaborative Research Working Group. Eur Urol 78: 21–24. [View]
- CompératE (2020) What Does COVID-19 Mean for the Pathology-Urology Interaction. Eur Urol 78: 43–44. [View]
- Msurgery.ie
- https://www.rcseng.ac.uk/coronavirus/recovery-of-surgical-services/