- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Constructing An online Information System for Infectious Disease: Increasing both Patient and Healthcare Worker Safety During Radiotherapy
- Home
- Back to Journal
- Article Details
Abstract
Purpose: Patients with cancer are vulnerable to infectious disease, especially that receiving combination therapy. However, preventing cross-infection during radiotherapy is time-consuming and challenging. This study aimed to construct an online information system to monitor both patient and healthcare worker safety during radiotherapy.
Methods: We establish a platform that integrated hospital information and radiation therapy systems. From January 2017 to December 2018, we collected information on 27,643 person-times of treatment with radiation to review the effectiveness of the newly developed system.
Results: After the interventions, the success rate for preventing infections increased to 94%, versus 14% before the interventions (p < 0.001). After further optimization, the success rate was improved to 100%. Treatment confidence among radiotherapy team members was increased markedly from 2.6 to 4.2 (p < 0.05). In addition, the time needed for monitoring and medical costs were reduced.
Conclusion: The integrated information system can increase both patient and healthcare worker safety during radiotherapy.
Keywords: Cross-infection, Information System, Radiotherapy, Safety
Introduction
Cancer treatment often requires multiple modalities. Patients with cancer are vulnerable to infectious disease, especially patients receiving chemotherapy [1]. In the clinic, 40–60% of patients with cancer receive radiation therapy as part of their cancer treatments [2, 3]. However, radiation therapy systems are closed systems. Thus, it is a challenge to confirm the condition of patients during radiotherapy in a timely manner. Several studies revealed that concurrent chemoradiotherapy significantly improved survival but also increased the incidence of toxic effects, especially rates of infection, compared with radiation alone [4, 5]. Combination therapy often causes illnesses of varying complexity. Although patients must be followed up at outpatient departments weekly during radiotherapy, a well-established platform connecting physicians, patients, and frontline technologists is not available [6]. Thus, we attempted to establish an online information system that can integrate hospital information and radiation therapy systems and provide physicians and technologists with immediate information concerning possible infectious disease among patients receiving radiotherapy. In this study, we evaluated the feasibility of computer-aided monitoring and reviewed its effectiveness.
Materials and Methods
Ethics statement
The study protocol was approved by the Institutional Review Board of Buddhist Dalin Tzu Chi Hospital (no. B10403001). The procedures of the study were conducted in accordance with both the ethical standards of the Institutional Review Board of our institution and the Declaration of Helsinki.
Integrated information system
We established a platform that can integrate hospital information and radiation therapy systems (Figure 1). In brief, the integrated information system can connect hospital information and radiation therapy systems and automatically search for symptoms of infectious disease. If patients met the criteria of the integrated information system, the computer-aided monitoring system notified physicians and frontline technologists to provide appropriate management. For example, if radiotherapy-treated patients developed tubercle bacillus infection, the integrated system alerted physicians and frontline technologists, permitting them to take appropriate actions to prevent cross-infection (Table 1).
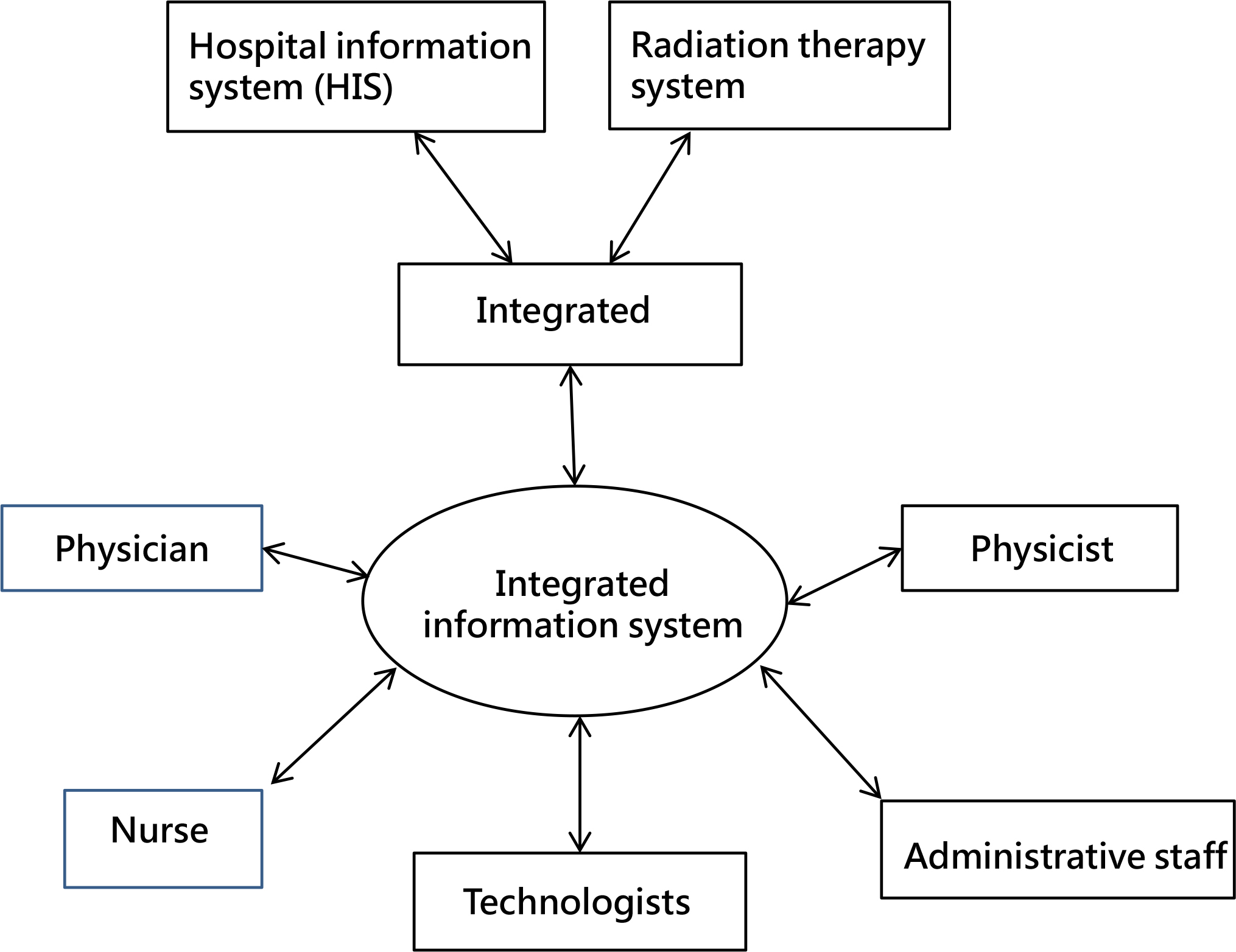
Figure 1: A flowchart illustrating the integrated information system architecture.
Table 1: Appropriate procedures for preventing cross-infection.
|
Isolation mode |
Protective procedure |
Common diseases |
|
Standard precaution |
|
|
|
Contact isolation |
|
gastrointestinal infections (Salmonella, Shigella, rotavirus) scabies, exudate/abscess/cellulitis, bedsores, viral hepatitis, multiple drug-resistant bacteria (MRSA, VRE, CRAB, CRPA, CRE), conjunctivitis, enterovirus, AIDS |
|
Droplet isolation |
|
invasive Haemophilus influenzae type B infection, whooping cough, scarlet fever, epidemic encephalitis, diphtheria of the throat, mumps, influenza virus, rubella |
|
Air isolation |
|
open pulmonary tuberculosis, measles, chicken pox, SARS |
Patients
From January 2017 to December 2017, we first retrospectively collected data for 21,188 person-times of treatment with radiation before the integrated information system was established. In addition, a questionnaire was used to confirm why frontline technologists failed to respond appropriately when patients met the criteria for infectious disease. From September 2018 to December 2018, we collected data for 6455 person-times of treatment with radiation after the integrated system was implemented to assess its effectiveness in preventing cross-infections. A questionnaire was also used to test treatment confidence after the system was implemented.
Statistical analysis
The SAS statistical package (version 9.2; SAS Institute, Inc., Cary, NC, USA) and SPSS (version 21, SPSS Inc., Chicago, IL, USA) were used for data analysis. Statistical analyses were performed using Fisher’s exact test to compare data for before and after implementation of the monitoring system. p < 0.05 denoted statistical significance.
Results
From January 2017 to December 2018, we identified 35 person-times of infection that required adequate infection control procedures during radiotherapy, but appropriate measures were employed for only 14% (5/35) of the cases. A questionnaire was used to determine why infection control procedures were not employed. The two major explanations were “inspection system did not send messages because of statutory infectious diseases” and “the alert-message-received department didn’t transfer the information to radiation department” (Figure 2). To solve these problems, we first conducted conferences and reached consensuses. Then, we integrated different systems to develop an online infection monitoring system. After implementing the monitoring system, pathogenic infection was identified 16 person-times over a 3-month follow-up period. Of these, adequate infection control procedures were adopted during radiotherapy in 94% (15/16) of the cases. Thus, the developed monitoring system dramatically increased the use of infection control procedures during radiotherapy (p < 0.001, Table 2). We worked to improve the system, and through December 2019, the rate at which adequate measures were adopted was improved to as high as 100%. Treatment confidence among radiotherapy team members also increased markedly (from 2.6 to 4.2; p < 0.05) after implementation of the monitoring system (Figure 3). We also checked the time required for patient monitoring. For manual monitoring, 40 min were needed per 100 patients per day. If we used the newly developed monitoring system, all patients could be checked in approximately 1 min. After further improvements, the display was divided into different treatment rooms, and the monitoring time of the system was shortened to 25 s (Figure 4).
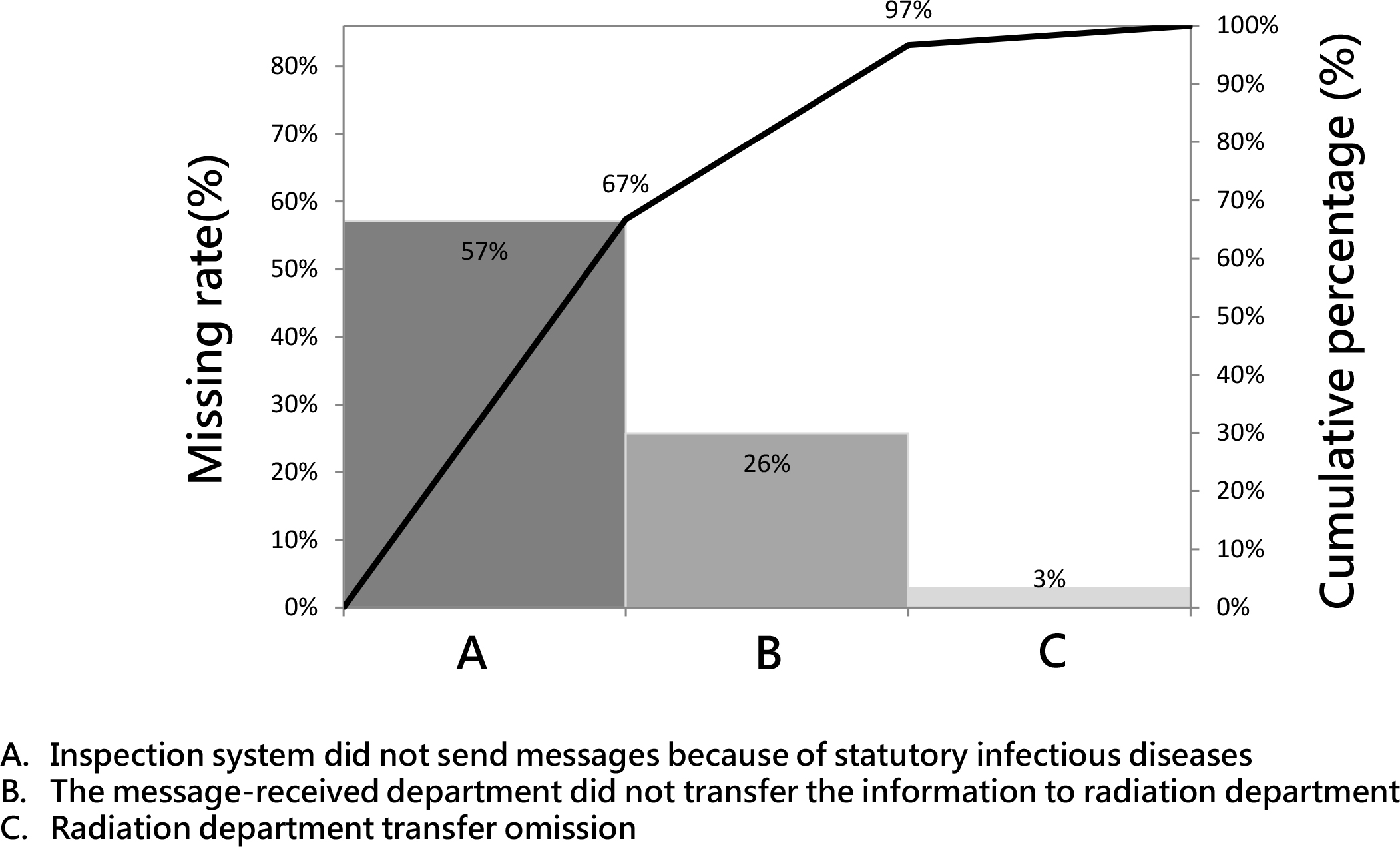
Figure 2: The standard protection guidelines.
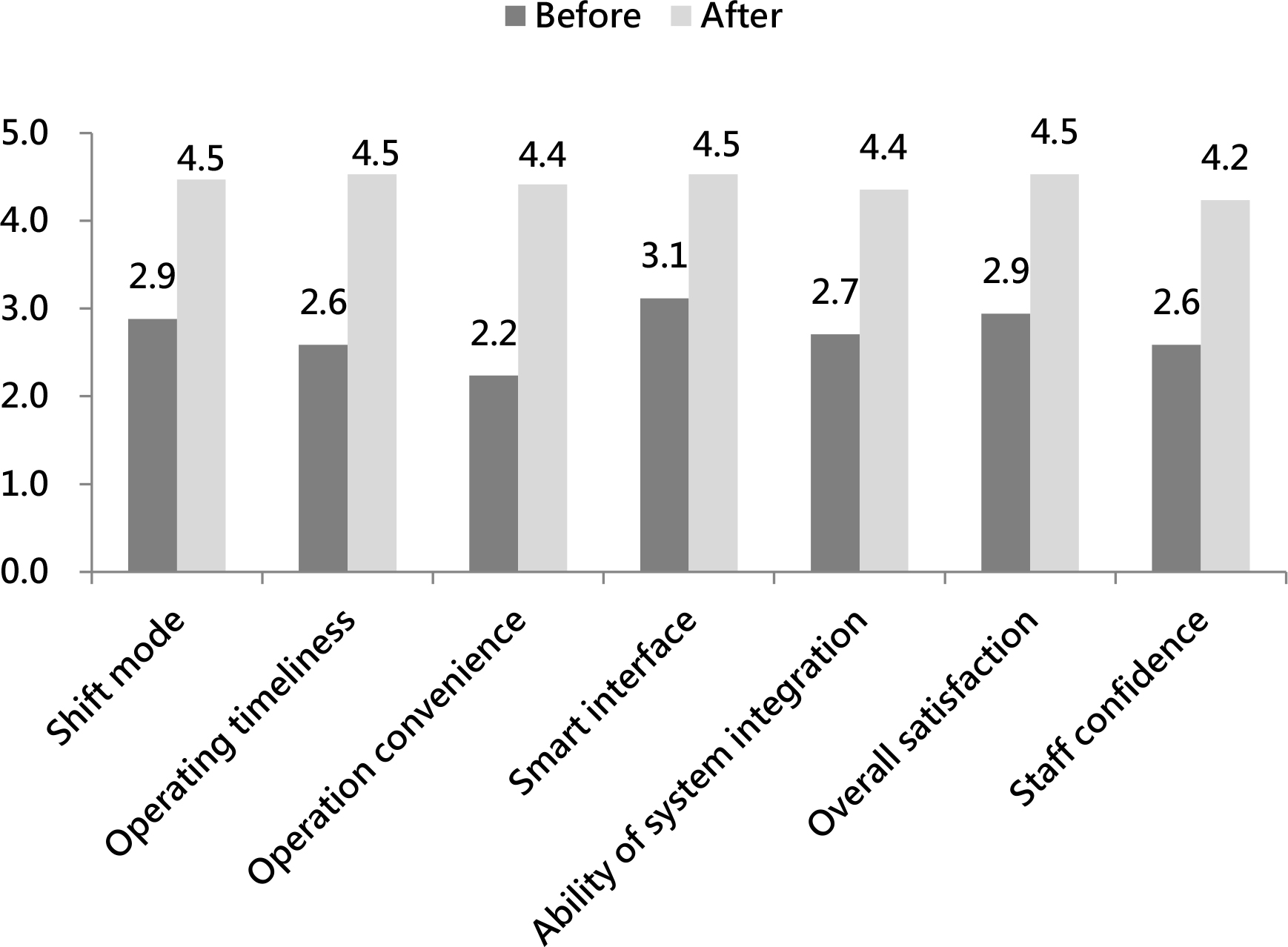
Figure 3: The figure of Plato presents the reasons why patients who met the criteria for infectious disease were not provided protective modalities.
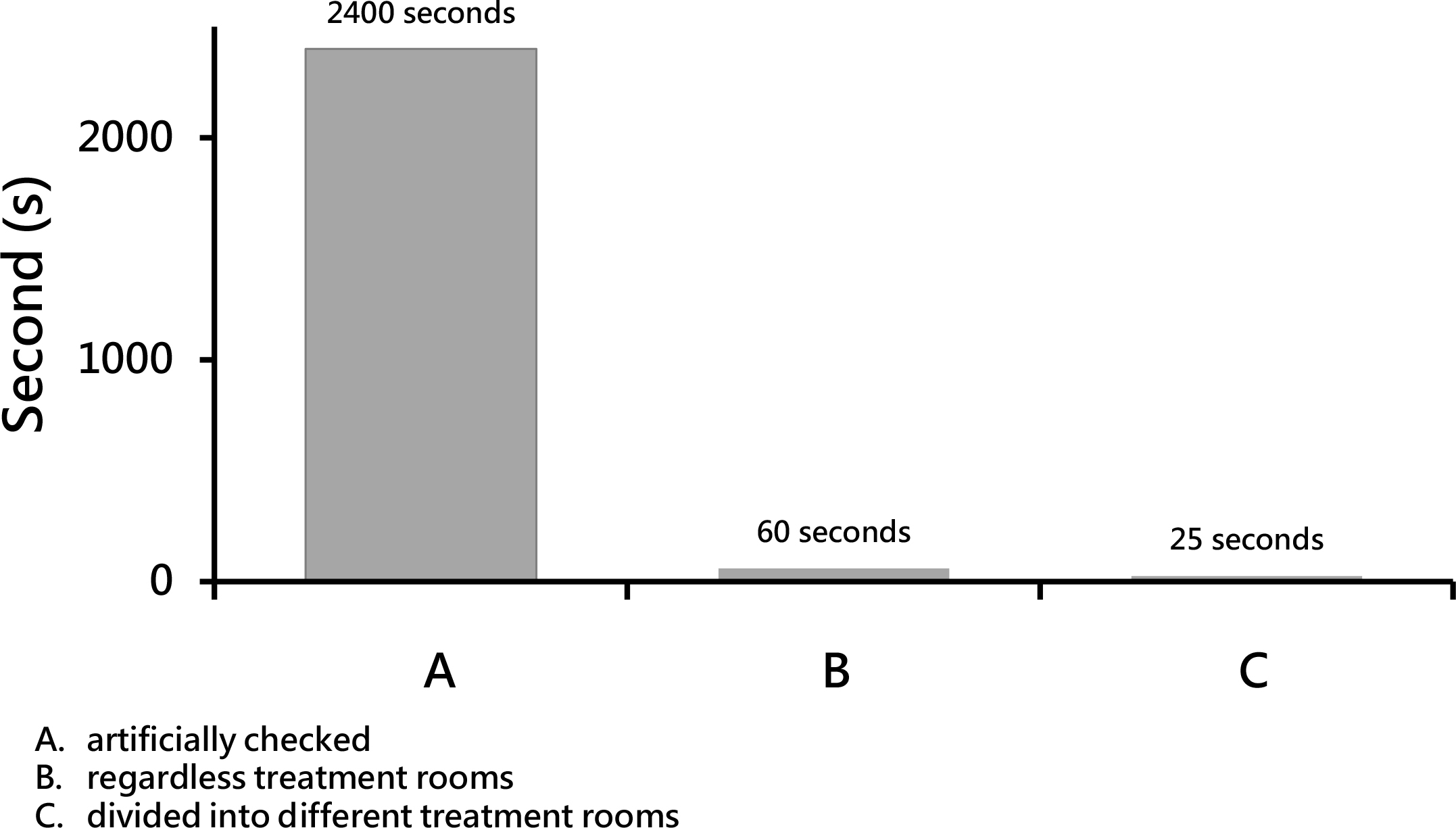
Figure 4: The ratio of treatment confidence among healthcare workers.
Table 2: The numbers of patients for whom infection-preventing measures were adopted during radiotherapy before and after implementation of the monitoring system.
|
|
Number of patients |
Adoption of adequate protection |
Non-adoption of adequate protection |
*p value |
|
Before |
35 |
5 |
30 |
<0.0001 |
|
After |
16 |
15 |
1 |
|
Discussion
The safety of patients and frontline staff regarding the administration of radiotherapy is a dynamic concept that must be considered and measured using scientific methods and feedback by the treatment teams [7]. In addition to quality assurance and treatment parameters to ensure that patients receive the safest precise therapeutic dose, methods for immediately communicating information in an interdisciplinary environment are increasingly important [8, 9]. For example, healthcare workers may serve as vectors of many infectious diseases, many of which are not generally considered to be healthcare-associated [10]. Infection transmission may result in morbidity and mortality among patients and frontline staff. To minimize the risk of infection transmission, standard infection control precautions must be employed [11]. In addition to training, the most important issue is providing timely and accurate information to healthcare workers. Radiation therapy systems are closed systems. Thus, it is difficult to for radiotherapy teams to communicate with other departments. In this study, we integrated hospital information and radiation therapy systems. This integrated platform could provide timely and accurate information and allow healthcare workers to provide appropriate management. As a result, we improved response rates and decreased the time required for patient monitoring.
To ensure patient and frontline staff safety during radiotherapy, infection transmission must be stopped to prevent new infections [12]. Active case finding and real-time management need to be aggressively implemented. Several studies demonstrated that timely interventions could effectively reduce infection rates and treatment costs [13, 14]. In this study, the response rate was improved from 14 to 94%. After further improvements, the rate was increased to as high as 100%. The National Health Insurance covers medical benefit claims for 97% of the population in Taiwan [15], resulting in large workloads among Taiwanese physicians. An excessive workload could result in shortages of medical resources and affect patient safety [16]. Thus, strategies are needed to maintain medical quality and reduce physicians’ workloads in Taiwan. We can increase treatment efficiency and reduce manual labor by using the developed monitoring system. In this study, we reduced labor costs by approximately 12.5%. In addition, reducing physicians’ workloads will also improve the hospital environment and patient-physician relationships [17].
Members of the radiotherapy team include physicians, nurses, physicists, technologists, and administrative staff. The successful completion of radiotherapy requires expertise, training, and coordination in an team-oriented environment [7]. To ensure that the integrated system functioned properly, we held several conferences and reached consensuses. Because the warning system can notify the proper target, standard guidelines have been established. Technology can increase efficiency, reduce workloads, and improve patient and frontline staff safety. We have developed the first real-time online system for monitoring infection status during radiotherapy in Taiwan. In addition, this integrated information system could have additional applications. First, integrated information system can monitor important risk values, such as blood or biochemical data. This application can allow frontline physicians to provide complete monitoring for patients during radiotherapy. Second, as radiotherapy treatment systems are closed systems, it is difficult for other treatment teams to obtain real-time or complete information during radiotherapy. This integrated system provides a platform that can convey information to different groups. Third, the complete integrated system can be used as electronic medical records system to achieve the goal of a paperless environment [18].
In conclusion, we have established an integrated information system. This system can increase both patient and frontline staff safety during radiotherapy.
References
- Sasaki T, Takenaka Y, Hayashi T, Yamamoto M, Cho H, et al. (2015) Factors predicting severe infections during chemotherapy in head and neck cancer patients. Acta Otolaryngologica 135: 1086–1091. [View]
- Sharma S, Hertan L, Jones J (2014) Palliative radiotherapy: current status and future directions. Seminars in Oncology 41: 751–763. [View]
- Baskar R, Lee KA, Yeo R, Yeoh KW (2012) Cancer and radiation therapy: current advances and future directions. Int J Med Sci 9: 193–199. [View]
- Park J, Ahn YC, Kim H, Lee SH, Park SH, et al. (2003) A phase II trial of concurrent chemoradiation therapy followed by consolidation chemotherapy with oral etoposide and cisplatin for locally advanced inoperable non-small cell lung cancers. Lung Cancer 42: 227–235. [View]
- Wu SY, Wu YH, Yang MW, Hsueh WT, Hsiao JR, et al. (2014) Comparison of concurrent chemoradiotherapy versus neoadjuvant chemotherapy followed by radiation in patients with advanced nasopharyngeal carcinoma in endemic area: experience of 128 consecutive cases with 5 year follow-up. BMC Cancer 14: 787. [View]
- Wang X, Jin J, Li YX, Ren H, Fang H, et al. (2014) Phase I study of postoperative radiotherapy combined with capecitabine for gastric cancer. World J Gastroenterology 20: 1067–1073. [View]
- Papakostidi A, Tolia M, Tsoukalas N (2014) Quality assurance in Health Services: the paradigm of radiotherapy. J BUON 19: 47–52. [View]
- Reinhart R, D’Alimonte L, Osmar K, Court A, Szumacher E, et al. (2014) Educating our patients collaboratively: a novel interprofessional approach. J Cancer Educ 29: 382–388. [View]
- Valentini V, Glimelius B, Frascino V (2013) Quality assurance and quality control for radiotherapy/medical oncology in Europe: guideline development and implementation. Eur J Surg Oncol 39: 938–944. [View]
- Huttunen R, Syrjanen J (2014) Healthcare workers as vectors of infectious diseases. Eur J Clin Microbiol Infect Dis 33: 1477–1488. [View]
- Ritchie L, McIntyre J (2015) Standardising infection control precautions. Nurs Times 111: 17–20. [View]
- Yuen CM, Amanullah F, Dharmadhikari A, Nardell EA, Seddon JA, et al. (2015) Turning off the tap: stopping tuberculosis transmission through active case-finding and prompt effective treatment. Lancet 386: 2334–2343. [View]
- Beam EL, Gibbs SG, Hewlett AL, Iwen PC, Nuss SL, et al. (2014) Method for investigating nursing behaviors related to isolation care. Am J Infect Control 42: 1152–1156. [View]
- Luangasanatip N, Hongsuwan M, Limmathurotsakul D, Lubell Y, Lee AS, et al. (2015) Comparative efficacy of interventions to promote hand hygiene in hospital: systematic review and network meta-analysis. BMJ 351: h3728. [View]
- Lee MS, Tsai SJ, Lee CC (2014) Higher caseload improves cervical cancer survival in patients treated with brachytherapy. Radiat Oncol 9: 234. [View]
- Chen KY, Yang CM, Lien CH, Chiou HY, Lin MR, et al (2013) Burnout, job satisfaction, and medical malpractice among physicians. Int J Med Sci 10: 1471–1478. [View]
- Wu H, Sun W, Wang L (2012) Factors associated with occupational stress among Chinese female emergency nurses. Emerg Med J 29: 554–558. [View]
- Kirkpatrick JP, Light KL, Walker RM, Georgas DL, Antoine PA, et al. (2013) Implementing and integrating a clinically driven electronic medical record for radiation oncology in a large medical enterprise. Front Oncol 3: 69. [View]